Group A streptococcal infections: report on seasonal activity in England, 2021 to 2022 - GOV.UK
Main points
Scarlet fever surveillance is showing an increase in recent notification levels in line with usual seasonal pattern, also reflected in weekly GP consultation data. Notifications have been very low since March 2020, reflecting measures to curb transmission of SARS-CoV-2. Concurrent increases have been noted in chickenpox consultations, again reflecting a seasonal rise typical for this time of year.
Due to the coronavirus (COVID-19) pandemic there has been very little chickenpox activity in the last 2 seasons and so a larger pool of susceptible children have accrued during this period.
The number of laboratory notifications of invasive group A streptococcal (iGAS) disease are below average compared to the past 4 seasons, but showing a usual seasonal increase.
While increases in severe presentations in children have not been seen so far this season, it remains important that scarlet fever cases are treated promptly with antibiotics to limit further spread, and reduce risk of potential complications in cases and household contacts.
Due to these uncommon but potentially severe complications associated with GAS infections, clinicians (and health protection teams, or HPTs) should continue to be mindful of potential increases in invasive disease and maintain a high degree of clinical suspicion when assessing patients, particularly those with preceeding chickenpox or close contacts of scarlet fever.
As per national guidance, prompt notification of scarlet fever cases and outbreaks to local UK Health Security Agency (UKHSA) HPTs, obtaining throat swabs (prior to commencing antibiotics) when there is uncertainty about the diagnosis, and exclusion of cases from school or work until 24 hours of antibiotic treatment has been received remain essential tools to limit spread.
Scarlet fever
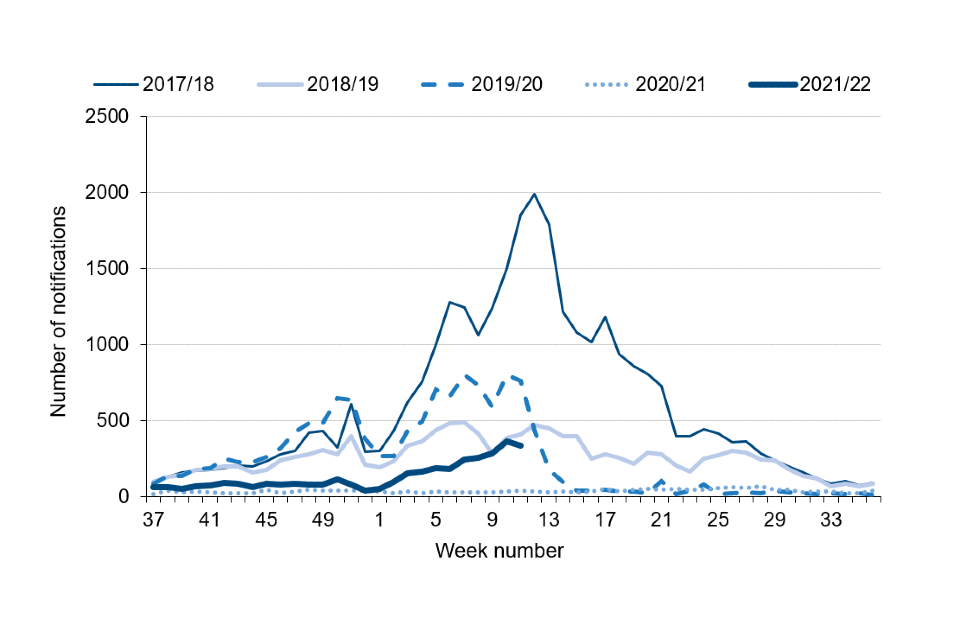
After low levels of activity at the start of the season, scarlet fever notifications in England are increasing in line with the usual seasonal pattern (figure 1). A total of 3,488 notifications of scarlet fever have been received to date this season in England (between week 37 of 2021 and week 11 of 2022) compared to an average of 8,605 (range 787 to 15,466) for this same period in the previous 5 years.
Weekly notification totals of 280 and 361 were recorded in the 2 most recent complete weeks (weeks 9 and 10). A provisional total of 333 notifications were made for week 11, with the potential for late reports to still be received.
The last (2020 to 2021) season remained exceptionally low in numbers, with only 1,791 notifications being recorded across the 12 months. This contrasts with prior seasons where higher numbers of notifications were recorded (30,768 in 2017 to 2018; 13,395 in 2018 to 2019; and 12,934 in 2019 to 2020).
Figure 1. Weekly scarlet fever notifications in England, 2017 to 2018 onwards
Scarlet fever notifications to date this season showed considerable variation across England, ranging between 1.5 (South West) and 12.4 (North West) per 100,000 population (Table 1). After the North West the highest observed rates were in North East (11.2), Yorkshire and the Humber (9.9) and the East Midlands (9.4) regions.
Table 1. Counts and rate per 100,000 population of scarlet fever (weeks 37 to 11) and iGAS (weeks 37 to 10) notifications in England: 2021 to 2022
| UKHSA centre name | Number of cases of scarlet fever | Rate of scarlet fever | Number of cases of iGAS | Rate of iGAS |
|---|---|---|---|---|
| East of England | 355 | 5.3 | 53 | 0.8 |
| East Midlands | 458 | 9.4 | 40 | 0.8 |
| London | 319 | 3.5 | 39 | 0.4 |
| North East | 301 | 11.2 | 46 | 1.7 |
| North West | 914 | 12.4 | 89 | 1.2 |
| South East | 282 | 3.2 | 75 | 0.8 |
| South West | 83 | 1.5 | 32 | 0.6 |
| West Midlands | 230 | 3.9 | 59 | 1.0 |
| Yorkshire and the Humber | 546 | 9.9 | 72 | 1.3 |
| England | 3,488 | 6.2 | 505 | 0.9 |
The age distribution of scarlet fever cases notified so far for this season remains similar to previous years, with 89% being children under 10 years (median 4 years; range <1 year to 103 years).
Invasive group A streptococcal infection
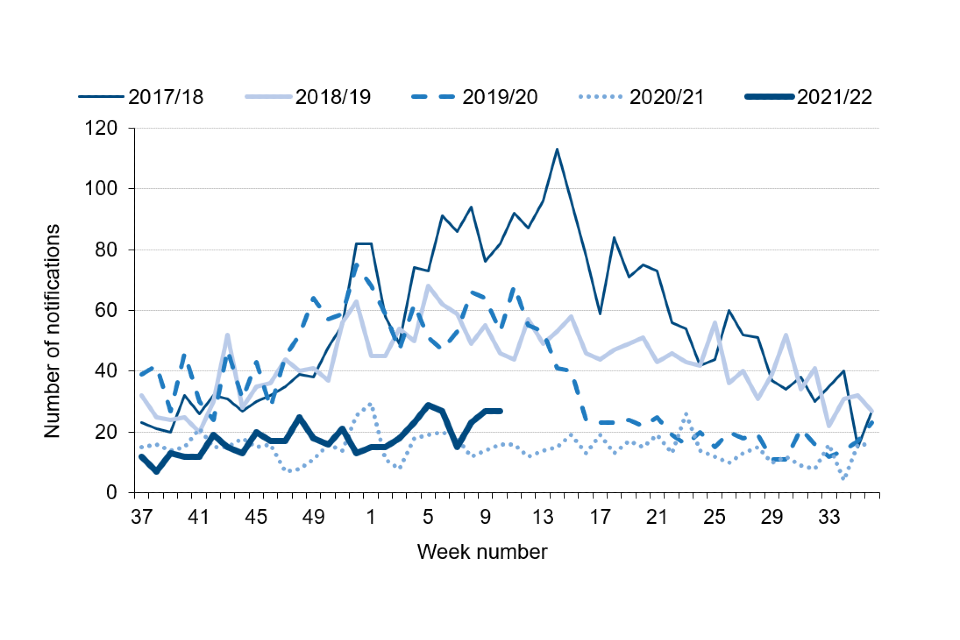
So far this season (week 37 to 10 of the 2021 to 2022 season), there have been 505 notifications of iGAS disease reported through laboratory surveillance in England, lower than the average (1,080) for the previous 5 years (range 780 to 1,315: see figure 2).
The total iGAS notifications recorded in the 2020 to 2021 season was exceptionally low at only 773, and the prior season (2019 to 2020) noted a large reduction mid way through (decreasing 55% between weeks 12 and 16), coinciding with the first wave of the COVID-19 pandemic.
The total number of laboratory iGAS notifications recorded in the seasons since 2017 to 2018 showed successive decline, from 2,875 in 2017 to 2018, to 2,234 in 2018 to 2019 and 1,929 in 2019 to 2020 (figure 2).
In the current season, the highest rates so far were reported in the North East region (1.7 per 100,000 population), followed by the Yorkshire and Humber (1.3 per 100,000) and North West (1.2 per 100,000) regions. All region except for the South West and London regions had higher rates compared to the same point last season.
Figure 2. Weekly laboratory notifications of invasive GAS, England, 2017 to 2018 season onwards
The median age of patients with iGAS infection so far this season is 53 years (range <1 year to 102 years), which is slightly lower than the range seen at this point in the preceding 4 seasons (56 to 57 years). Twelve per cent of infections reported this season are in children (<10 years), which is within the normal range seen for the past 4 seasons (10% to 14%, excluding the 2020 to 2021 season which recorded only 4% in children).
Analysis of reference laboratory iGAS isolate submissions indicate a diverse range of emm gene sequence types identified between January and March 2022. The results indicate the emm 89 are the most common (11% of referrals), followed by emm 108 (10%), emm 77 (9%), emm 1 and emm 12 (each 8%).
During 2021, emm 89 was the most frequently identified (13%), followed by emm 108 (12%) then emm 66 (11%). This indicates that there has been a change in the dominant emm type and increase in the diversity in isolates being referred compared with what has been reported in pre-pandemic seasons.
Antimicrobial susceptibility results from routine laboratory surveillance so far this season (September 2021 to February 2022) indicate erythromycin resistance in 17% of GAS sterile site isolates, higher than at the same point in the previous few seasons (7% to 8%).
An increase in tetracycline resistance has been noted this season (42%) compared to last season (40%), this continues an increasing trend in resistance over the last 5 seasons (13% at this point in the 2017 to 2018 season).
Susceptibility testing of iGAS isolates against clindamycin demonstrated 14% resistance at this point in the season (compared with 10% last season), and isolates remained universally susceptible to penicillin.
Discussion
The early part of the season remained low for scarlet fever notifications, compared with what was being reported pre-pandemic (2018 to 2019 season).
A gradual increase in notifications and GP consultations for scarlet fever seen in recent weeks align with would be expected at this point within the season, where peak activity typically occurs between weeks 11 and 15 (mid-March to mid-April). This contrasts with what was seen during the COVID-19 pandemic (2020 to 2021 season) where a slight increase was noted in the summer rather than the normal spring seasonal increase.
These changes are most likely as a result of the measures implemented at that time to reduce transmission in schools and wider society, including limiting mixing and use of masks and other control measures, as well as the withdrawal of such measures (1).
Prompt treatment of scarlet fever with antibiotics is recommended to reduce risk of possible complications and limit onward transmission. Renewed messaging to encourage contact with GP practices for patients with specific symptoms (for example, rash), should be considered. GPs and other frontline clinical staff are reminded of the increased risk of invasive disease among household contacts of scarlet fever cases (2, 3).
The number of cases of iGAS disease notified through routine laboratory surveillance in England is slightly elevated compared with the same point last season (2020 to 2021), but lower than what was seen prior to the COVID-19 pandemic.
There has been no notable increase in paediatric cases of iGAS, however vigilance is warranted given the elevated levels of chickenpox co-circulating.
Clinicians, microbiologists and HPTs should continue to be mindful of potential increases in invasive disease and maintain a high index of suspicion in relevant patients as early recognition and prompt initiation of specific and supportive therapy for patients with iGAS infection can be life-saving.
Invasive disease isolates and superficial isolates from suspected clusters or outbreaks should be submitted to:
The Staphylococcus and Streptococcus Reference Section
Antimicrobial Resistance and Healthcare Associated Infections (AMRHAI) unit
UK Health Security Agency
61 Colindale Avenue
London NW9 5HT
Prepared by: Rebecca Guy, Kirsty Bennet, Juliana Coelho, Colin Brown and Theresa Lamagni.
For queries relating to this document, please contact hcai.amrdepartment@phe.gov.uk
References
1. Chudasama D and others (2021) 'Surge in SARS-CoV-2 transmission in school-aged children and household contacts, England, August to October 2021', Eurosurveillance: volume 26, number 48
2. Lamagni T and others (2018) 'Resurgence of scarlet fever in England, 2014 to 2016: A population-based surveillance study', The Lancet Infectious Diseases: volume 18, number 2, pages 180 to 187
3. Watts V and others (2019) 'Increased risk for invasive group A Streptococcus disease for household contacts of scarlet fever cases, England, 2011 to 2016', Emerging Infectious Diseases: volume 25, number 3, pages 529 to 537

Comments
Post a Comment