What is your meningitis vaccine IQ? - Contemporary Pediatrics
Knowing which vaccines prevent meningitis and meningococcal disease and sharing the information with adolescents and caregivers are crucial responsibilities of all pediatric health care providers. Below are the things you need to know about this group of diseases and the vaccines available to prevent them. You can access the Centers for Disease Control and Prevention (CDC) immunization schedules for pediatric patients here.
Invasive bacterial meningitis
Invasive bacterial meningitis is a devastating disease that presents suddenly in the pediatric population. Irrespective of the organism causing it, infected newborns and infants most often exhibit behavioral changes, including unexpected changes in feeding patterns, difficulty sucking and/or feeding, vomiting, irritability, and lethargy.1,2,3 Infants may present with abnormal reflexes, and children with nuchal rigidity, fever, headache, nausea with or without vomiting, photophobia, and altered mental status.1,2 Adolescents and young adults may present with a progressively severe headache and flu-like symptoms, fever, nuchal rigidity, vomiting, fatigue, and a petechial rash that may progress to purpura.4
Haemophilus influenza serotype type b (Hib) is a bacterial disease that primarily affects infants and children less than 5 years old.1-4 Unvaccinated or partially vaccinated healthy newborns, infants, children under 5, and those with specific chronic illnesses (sickle cell disease, asplenia, human immunodeficiency virus [HIV]) or receiving chemotherapy for cancer are susceptible to invasive Hib infections.1,2 The Hib pathogen spreads via respiratory droplets from symptomatic or asymptomatic individuals who harbor the organism in their nose or throat.1,2 Even with immediate diagnosis and treatment, children with Hib meningitis may not survive or may experience long-term adverse effects, including hearing loss and brain damage.1,5,6
Streptococcus pneumoniae causes purulent invasive bacterial pneumococcal meningitis in infants and young children. In the United States, this type of meningitis is most commonly seen in children between the ages of 2 months and 11 years7 and is the leading cause of bacterial meningitis in children less than 5 years old. S pneumoniae is often spread by an asymptomatic nasopharyngeal carrier via respiratory droplets, and its incubation period can be as short as 1 day.7,8 In addition, transmission may occur through autoinoculation in individuals who carry the bacteria in their upper respiratory tract.9 According to the CDC, 5% to 10 % of adults without children and as many as 20% to 60% of school-aged children may be carriers of the disease.9 Infants, preschoolers, and school-aged children are all highly susceptible to viral upper respiratory tract infections, including influenza, which may make them vulnerable to S pneumoniae disease that may rapidly progress to pneumonia or meningitis. Infants and young children with S pneumoniae meningitis may show cranial nerve signs or seizures and may slip into a coma. Neurological sequalae occur in approximately 50% of survivors and can include changes in intellectual function, new-onset behavioral disabilities, seizures, hearing loss, and motor deficits.7 The case fatality rate for pneumococcal meningitis is approximately 8% in the pediatric population.9
Meningococcal infections
Caused byNeisseria meningitidis,10 invasive meningococcal infections present as meningococcemia (in approximately 50% of cases) and septicemia (in 30% to 40%),anda child may present with both conditions.11 About 1 in 10 individuals are asymptomatic carriers, meaning that they harbor the organism in the back of their nose and throat and can spread it via nasal or oral secretions (eg, kissing or sharing water bottles and toothbrushes).11 Awareness of transmission route must be part of routine anticipatory guidance for all school-aged children and adolescents, especially those who participate in sports and regularly share water bottles.
Newborns and infants may not present with the classic symptoms of meningococcal meningitis10 but instead with a bulging anterior fontanelle.12 Infants, children, and adolescents with meningococcemia appear critically ill, and their symptoms include abrupt onset of fever, chills, malaise, myalgia, limb pain, and a macular or maculopapular rash that quickly transitions to petechial or purpuric rash.12
In addition, children and adolescents with meningococcal septicemia present with cold hands and feet, severe aches or pain in the muscles, joints, chest, or abdomen consistent with bacteria in the bloodstream that damage vascular walls and result in bleeding into the skin and internal organs.12,13 Nineteen percent of individuals who survive meningococcal disease will experience life-long sequelae, including but not limited to hearing loss, neurological disability, digit or limb amputation, skin scarring, new-onset neurological deficits (significant, lasting changes in cognitive abilities as evidenced by deviation from usual school performance and new-onset behavioral problems).10
Even with prompt diagnosis and aggressive antibiotic treatment, 15% of affected individuals will succumb to the disease.10,13 Increased intracranial pressure is often associated with meningococcal meningitis and most frequently diagnosed in severe and/or fatal cases.10
Vaccines against meningitis and meningococcus
The Hib vaccine protects infants and children aged less than 5 years from invasive Hib meningitis and other invasive Hib diseases (pneumonia, bacteremia, epiglottis, septic arthritis, cellulitis, otitis media, and purulent pericarditis).2 The earliest age at which this vaccine may be administered is 6 weeks (Table 1).
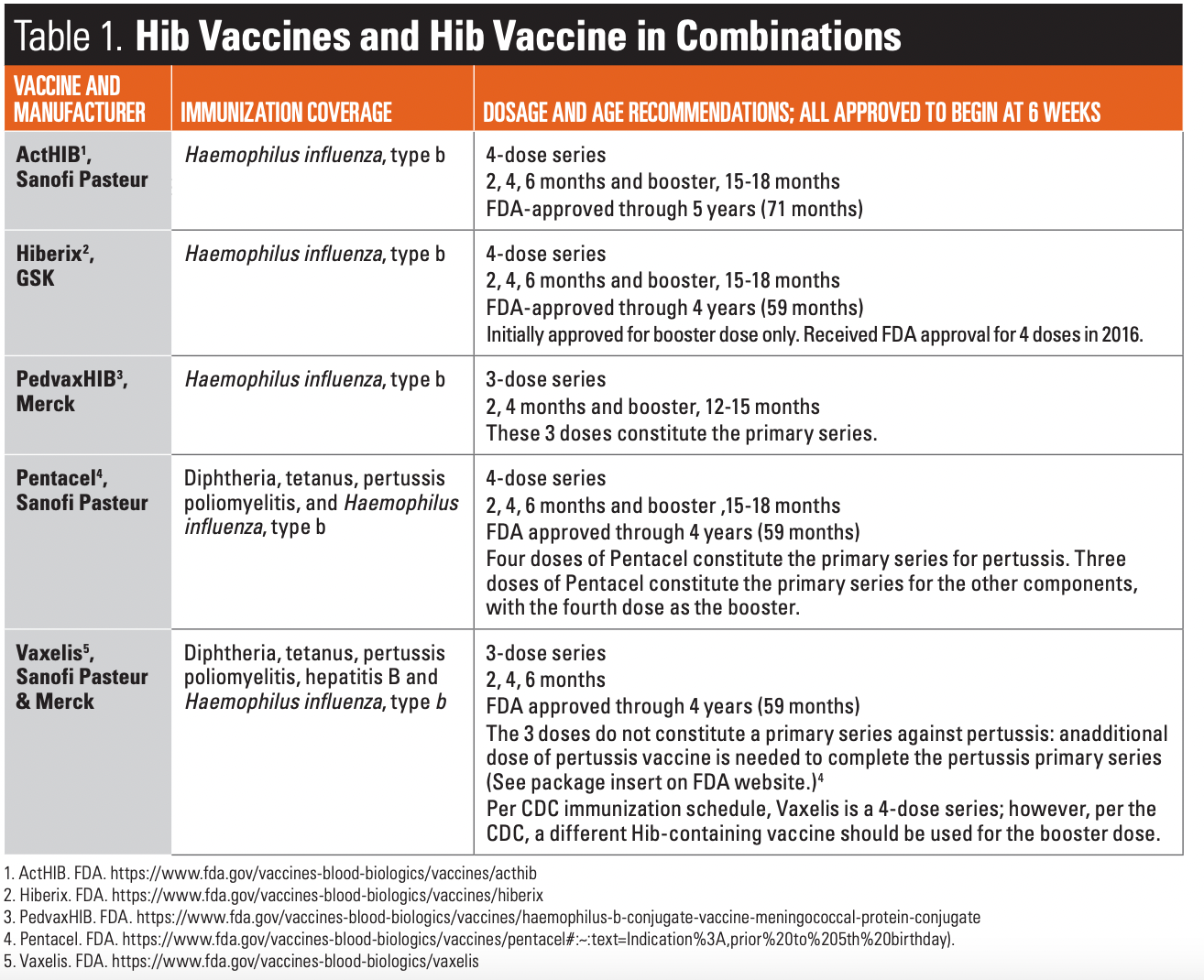
Prior to the licensing of the first Hib conjugate vaccine in 1987,14 invasive Hib disease was the most common cause of bacterial meningitis in children under 5 in the United States.1 The Hib conjugate vaccines administered as part of the routine CDC immunization schedule15 were a major public health success, with the incidence of invasive Hib disease decreasing more than 99% in children less than 5 years.4 Today, the nontypeable H influenza organism,which is not covered by the Hib vaccines, is the most common cause of invasive H influenza infections in all age groups, although it most often affects newborns during the first 2 weeks of life and premature babies who have a positive culture at birth.1 Nontypeable H influenza is also the cause of an estimated 50% of acute and recurrent otitis media and sinusitis in children.2,4
Therefore, physicians, nurse practitioners, physician assistants, nurses, and all individuals who works with infants and young children must encourage parents to immunize their children against all vaccine-preventable diseases.
Vaccines against pneumococcal meningitis
The Prevnar 13 vaccine (PCV-13) protects infants and children under 5 from contracting invasive bacterial pneumococcal meningitis as well as other diseases caused by S pneumoniae(acute otitis media, sinusitis, community-acquired pneumonia, pediatric conjunctivitis, periorbital cellulitis, mastoiditis, endocarditis, pericarditis, neonatal sepsis, etc).7 The earliest age at which this vaccine may be administered is 6 weeks.
The initial US Food and Drug Administration (FDA) approval of Prevnar was granted for the heptavalent PCV-7, which protected against pneumococcal serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F. Widespread uptake of this vaccine led to what is known as replacement disease, in which serotypes not included in PCV-7 were causing pneumococcal disease.4 Thus, in 2010 the 13-valent pneumococcal conjugate vaccine (PCV-13) was introduced to target 6 additional serotypes (1, 3, 5, 6A, 7F, and 19A).4,7 Since the introduction of these 2 vaccines, racial disparities for disease burden in infants and young children have diminished in the US.7 However, Native American and Alaska Native pediatric populations remain at high risk for pneumococcal disease, with data showing a fourfold rate of disease in these groups compared with all children in the general population.7 The majority of disease in the indigenous populations are caused by 4 serotypes not currently contained in the PCV-13 vaccine:12F, 22F, 24F, and 35B.4,7
On June 22, 2022, the FDA approved the pneumococcal 15-valent conjugate vaccine for pediatric use.16If initiated with a lower valency (eg, PCV-13), this 4-dose series can be completed with Vaxneuvance (PCV-15).16 Only 1 dose of Vaxneuvance (PCV-15) is required per the catch-up vaccine schedule for children 2 through 17 years who have not received any other doses of PCV-13 (Table 2).
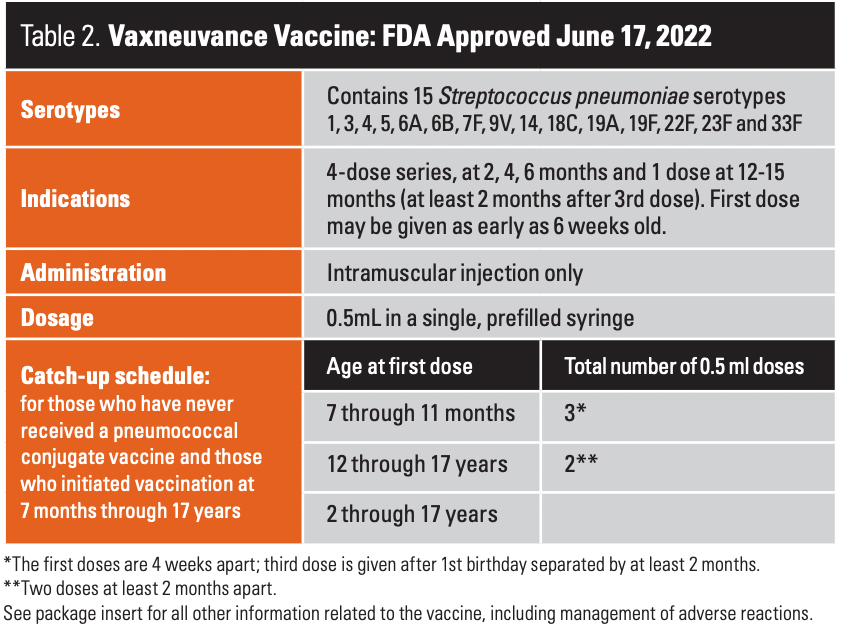
A study by Stevens et al17 urges practitioners to put S pneumoniae meningitis high on the list of differential diagnoses when an infant/young child presents with fever and altered mental status by history or examination and/or meningeal signs, e.g., headache, photophobia, neck stiffness, seizures. Additionally, there is a critical need for all health care providers to adhere to the CDC immunization schedule so as to protect all pediatric patients against diseases that are vaccine-preventable.15
Meningococcal vaccines
Pediatric primary care providers can prevent meningococcal disease in preteens and adolescents by discussing the value of immunization at every visit and providing strong support for adherence to the CDC schedule.15 Currently, there are 2 types of FDA-approved meningococcal vaccines in the US: meningococcal conjugate (MenACWY)18 and serogroup meningococcal (MenB).19
The MenB vaccine is on the immunization schedule; however, this vaccine, which protects against invasive meningococcal B disease and is recommended for college-age students who plan to live in dormitories, relies on shared decision-making (SDM)20 and is not required for school attendance. The Meningitis B Action Project offers a list of US colleges and universities that require or recommend the MenB vaccine for attendance.21 To date, only 45 colleges and universities mandate the vaccine.21 Of particular concern is the comparison of the list of schools that require the MenB vaccine to those that have had past MenB cases on their campuses between 2008 and May 2020.21 Even though several colleges and universities have had Men B disease cases on their campuses, they do not require the MenB vaccine.21 All pediatric/adolescent health care providers should consider recommending the MenB vaccine to all adolescents to reduce the annual incidence of the disease and protect them from invasive meningococcal meningitis, its long-term effects, and possibly even death.
Meningococcal serogroup ACWY
Although MenACWY is on the routine immunization schedule, only 34 states require it for school-aged children, which places millions of them are at-risk for an invasive vaccine-preventable disease.22 If an adolescent did not receive the MenACWY at 16-years-old, one dose of this vaccine is recommended for those entering college and planning to live in a dormitory(Table 3).22
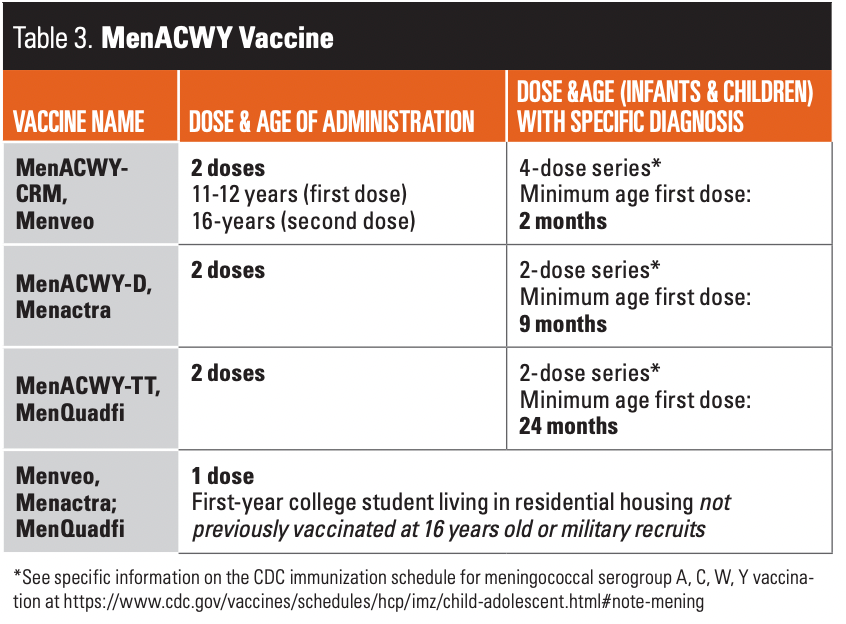
In addition, the vaccine is available for children with specific medical conditions like anatomic or functional asplenia, sickle cell disease, HIV infection, and persistent complement component deficiency and for those receiving complement inhibitors (eg, eculizumab, ravulizumab).15 Three MenACWY vaccines are available in the US. The MenACWY is administered to infants, toddlers, and young children with one of the conditions listed above based on the particular FDA approval.15 For example, these children can receive the first dose of Menveo (MenACWY-CRM) at 2 months; or Menactra (MenACWY-D) at 9 months or MenQuadfi (MenACWY-TT) at 24 months (Table 3).15 Infants and children with these medical conditions are often cared for in specialty centers. To prevent errors in, all providers should consult the CDC immunization schedule for children with medically complex conditions.15
Meningococcal serogroup B vaccine (MenB)
Two vaccines are licensed for meningococcal serogroup B disease prevention in the US: Trumenbaand Bexsero.23,24 The preferred age for these vaccines is between 16- to 18-years-old although it can also be administered between the ages of 16- to 23-years. The primary series and the booster dose of the available MenB vaccines are licensed for individuals 10-years old through 25-years old: The license for the 10-year-old through 15-years-old are for children with specific medical conditions.23,24 Health care providers who treat these children should be familiar with the CDC immunization schedule age-appropriate recommendations for these vaccines.
Safety and efficacy have not been established for children less than 10-years-old.
How many of the children in your practice are fully immunized against meningitis, including Haemophilus influenza serotype type b (Hib), S pneumoniae, meningitis ACWY, and meningitis B? One major benefit of the electronic medical record is that practice performance data can easily be extracted as an aggregate to analyze the number of patients eligible for a particular vaccine and the number who have received it. Only when such information is requested, made available, and analyzed can practice performance in terms of vaccine administration improve.
References
- Vaxneuvance. US Food and Drug Administration. July 22, 2022. Accessed July 22, 2022. https://www.fda.gov/vaccines-blood-biologics/vaccines/vaxneuvance
- Types of Haemophilus influenza infections.Centers for Disease Control and Prevention. March 4, 2022. Accessed July 19, 2022. https://www.cdc.gov/hi-disease/about/types-infection.html
- Haemophilus influenza disease (including Hib): signs and symptoms.Centers for Disease Control and Prevention. March 4, 2022. Accessed July 21, 2022. https://www.cdc.gov/hi-disease/about/symptoms.html
- Gierke R, Wodi P, Kobayashi M, eds. Epidemiology and prevention of vaccine-preventable diseases. The Pink Book. 14th ed. Centers for Disease Control and Prevention. Accessed July 21, 2022. https://www.cdc.gov/vaccines/pubs/pinkbook/pneumo.html#streptococcus-pneumoniae
- Kimberline DW, Barnett ED, Lynfield, R, Sawyer, MH, eds. Section 3. Summary of Infectious Diseases. In: Red Book: 2021–2024 Report of the Committee on Infectious Diseases. 32nd ed. American Academy of Pediatrics; 2021:345-354.
- Haemophilus influenza disease (including Hib): causes, how it spreads, and people at increased risk. Centers for Disease Control and Prevention. March 4, 2022. Accessed July 21, 2022. https://www.cdc.gov/hi-disease/about/causes-transmission.html
- Haemophilus influenza disease (including Hib): diagnosis, treatment and complications. Centers for Disease Control and Prevention. March 4, 2022. Accessed July 21, 2022. https://www.cdc.gov/hi-disease/about/diagnosis-treatment.html
- Kimberline DW, Barnett ED, Lynfield, R, Sawyer, MH, eds. Section 3. Summary of Infectious Diseases. In: Red Book: 2021–2024 Report of the Committee on Infectious Diseases. 32nd ed. American Academy of Pediatrics; 2021:717-721.
- Pneumococcal disease: Streptococcus pneumoniae. Centers for Disease Control and Prevention. January 27, 2022. Accessed July 22, 2022. https://www.cdc.gov/pneumococcal/clinicians/streptococcus-pneumoniae.html
- Pneumococcal disease: transmission. Centers for Disease Control and Prevention. January 27, 2022. Accessed July 22, 2022. https://www.cdc.gov/pneumococcal/clinicians/transmission.html
- Meningococcal disease: causes and how it spreads. Centers for Disease Control and Prevention. February 7, 2022. Accessed July 22, 2022. https://www.cdc.gov/meningococcal/about/causes-transmission.html
- Kimberline DW, Barnett ED, Lynfield, R, Sawyer, MH, eds. Section 3. Summary of infectious diseases. In: Red Book: 2021–2024 Report of the Committee on Infectious Diseases. 32nd ed. American Academy of Pediatrics; 2021:519-521.
- Meningococcal disease: signs and symptoms. Centers for Disease Control and Prevention. February 7, 2022. Accessed July 22, 2022. https://www.cdc.gov/meningococcal/about/symptoms.html
- Meningococcal disease: diagnosis, treatment and complications. Centers for Disease Control and Prevention. February 7, 2022. Accessed July 22, 2022. https://www.cdc.gov/meningococcal/about/diagnosis-treatment.html
- Oliver SE, Moro P, Blain AE. Epidemiology and prevention of vaccine-preventable diseases. Haemophilus influenza. The Pink Book. 14th ed. Centers for Disease Control and Prevention. August 18, 2021. Accessed February 2, 2023. https://www.cdc.gov/vaccines/pubs/pinkbook/hib.html#:~:text=production%20was%20minimal.-,The%20first%20Hib%20conjugate%20vaccine%20was%20licensed%20in%201987.,immunogenicity%2C%20particularly%20in%20young%20children
- Child and adolescent immunization schedule: recommendations for ages 18 years or younger, United States, 2022. Centers for Disease Control and Prevention. February 17, 2022. Accessed July 20, 2022. https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html
- FDA approves pneumococcal 15-valent conjugate vaccine for pediatric use. U.S.Pharmacist. July 19, 2022. Accessed July 22, 2022. https://www.uspharmacist.com/article/fda-approves-pneumococcal-15valent-conjugate-vaccine-for-pediatric-use#:~:text=FDA%20Approves%20Pneumococcal%2015%2DValent%20Conjugate%20Vaccine%20for%20Pediatric%20Use,-By%20staff&text=In%20a%20press%20release%20on,6%20weeks%20through%2017%20years
- Stevens JP, Lively A, Jerris R, Yildirim I, Lantis P. Recognition and outcomes of pneumococcal meningitis in 2 tertiary pediatric hospitals since the introduction of the 13-valent pneumococcal conjugate vaccine. Pediatr Emerg Care. 2022;38(1):e354-e359. doi:10.1097/PEC.0000000000002288
- Child and adolescent immunization schedule: meningococcal serogroup A, C, W, Y vaccination. Centers for Disease Control and Prevention. February 17, 2022. Accessed July 25, 2022. https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html#note-mening
- Child and adolescent immunization schedule: meningococcal serogroup B vaccination. Center for Disease Control and Prevention. February 17, 2022. Accessed July 26, 2022. https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html#note-mening
- Grad R, Légaré F, Bell NR, et al. Shared decision making in preventive health care: what it is; what it is not. Can Fam Physician. 2017;63(9):682-684.
- You need two types of meningitis vaccines. Meningitis B Action Project. 2022.Accessed July 23, 2022. https://meningitisbactionproject.org/
- State information: MenACWY vaccine mandates for elementary and secondary schools. Immunize.org. November 30, 2019. Accessed July 25, 2022. https://www.immunize.org/laws/menin_sec.asp
- Trumenba. US Food and Drug Administration. November 23, 2021. Accessed July 25, 2022. https://www.fda.gov/vaccines-blood-biologics/vaccines/trumenba
- Bexsero. US Food and Drug Administration. January 7, 2022. Accessed July 25, 2022. https://www.fda.gov/vaccines-blood-biologics/vaccines/bexsero

Comments
Post a Comment